High Blood Pressure: What Your Numbers Mean and Why It Is Called the Silent Killer
Nearly half of adults with high blood pressure do not know they have it. By the time it causes symptoms, it has often already caused damage.
High blood pressure, or hypertension, earns the label "silent killer" because it causes no symptoms while progressively damaging the heart, arteries, kidneys, and brain over years. As a cardiologist, I treat the end-stage consequences of uncontrolled hypertension regularly: heart failure, stroke, kidney failure requiring dialysis, and hypertensive retinopathy causing vision loss. In nearly every one of these patients, the blood pressure was elevated for years before the event that brought them to me. The damage is predictable and largely preventable. Understanding what your blood pressure numbers mean, and taking them seriously before they reach the emergency stage, is one of the most impactful things you can do for your long-term health.
According to the World Health Organization, hypertension affects 1.28 billion adults worldwide. Approximately 46 percent of adults with hypertension are unaware of their diagnosis. Of those who are diagnosed, a significant proportion are not adequately treated. This treatment gap represents an enormous preventable burden of cardiovascular disease globally.
Understanding the Numbers
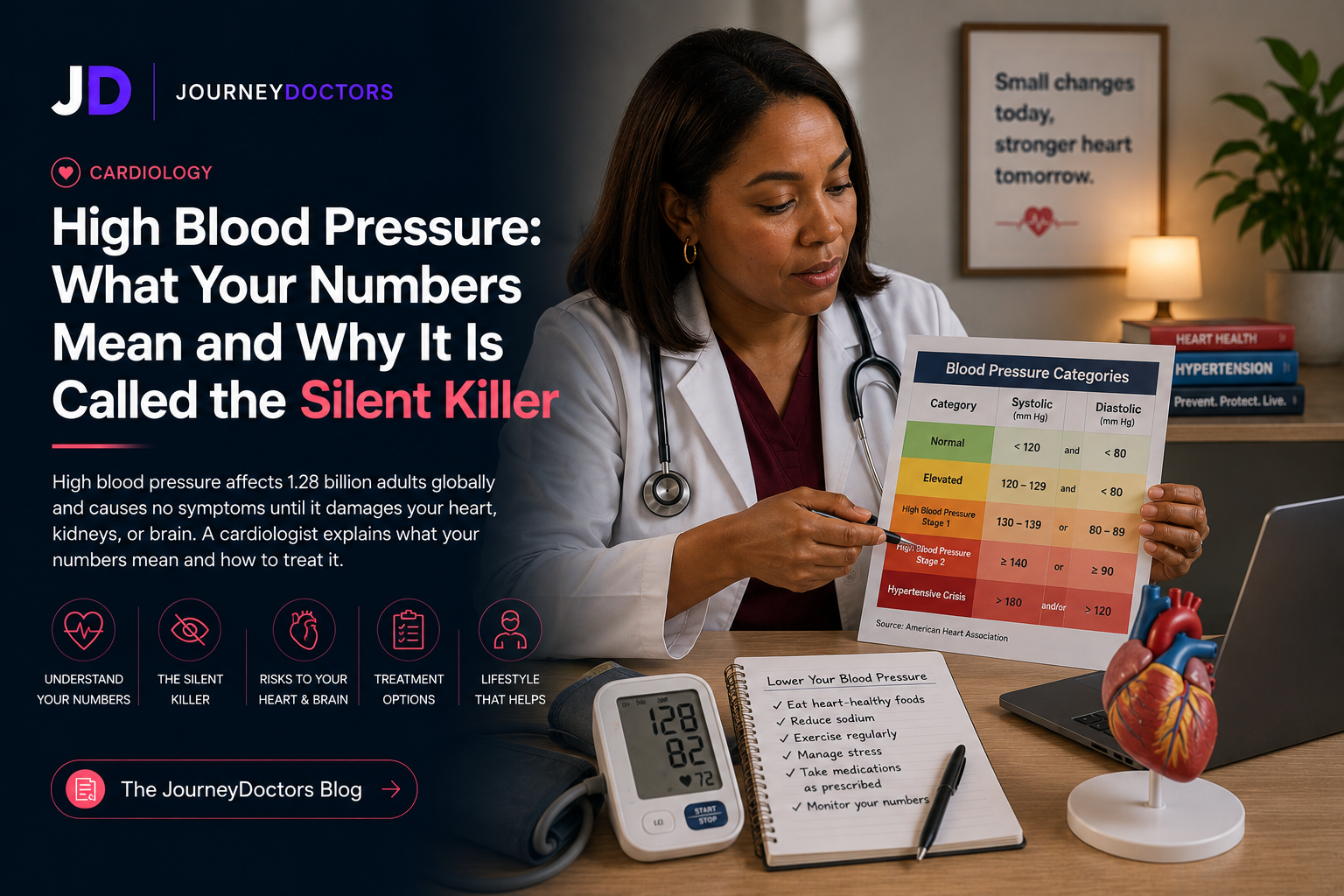
A blood pressure reading has two numbers. The top number, systolic pressure, measures the pressure in your arteries when your heart beats. The bottom number, diastolic pressure, measures the pressure between beats when your heart is at rest. Both matter, and both are used in assessing cardiovascular risk.
Current guidelines from major cardiology organizations define the categories as follows. Normal blood pressure is below 120/80 mmHg. Elevated blood pressure, sometimes called prehypertension, is a systolic of 120 to 129 with a diastolic below 80. Stage 1 hypertension is 130 to 139 systolic or 80 to 89 diastolic. Stage 2 hypertension is 140 or higher systolic or 90 or higher diastolic. Hypertensive crisis, which requires immediate medical evaluation, is a reading above 180/120 mmHg.
These thresholds are not arbitrary. Cardiovascular risk increases continuously above 115/75 mmHg; each 20 mmHg increase in systolic pressure doubles the risk of heart attack and stroke. The current definitions reflect where the evidence shows that intervention meaningfully reduces outcomes, not simply a line above which blood pressure is "bad."
Why Hypertension Causes No Symptoms
The arteries and heart adapt to elevated pressure gradually, accommodating the increased load over time without triggering pain or obvious dysfunction. This adaptation, while protective in the short term, allows the structural changes that drive long-term damage to occur silently.
The left ventricle of the heart thickens in response to having to pump against higher resistance, a process called left ventricular hypertrophy. The arteries stiffen and narrow. The kidneys, which are both regulators of blood pressure and victims of sustained elevation, progressively lose function. None of these changes announce themselves with symptoms until the system reaches a tipping point: a heart attack, heart failure, stroke, or kidney failure.
The absence of symptoms is exactly why routine blood pressure screening matters. Waiting to check your blood pressure until you feel unwell is waiting until the damage is already happening.
Causes and Risk Factors
JourneyDoctors
Not sure if this applies to you?
Describe your symptoms to Dr. Maya — our AI GP — and get a real clinical response in under a minute. Free to start.
Talk to Dr. MayaPrimary (Essential) Hypertension
Approximately 90 to 95 percent of hypertension cases are primary, meaning there is no single identifiable cause. Instead, primary hypertension results from a combination of genetic predisposition and lifestyle factors accumulating over years. Family history is one of the strongest predictors; if both parents had hypertension, the lifetime risk of developing it is approximately 60 percent. Older age, male sex (until women reach menopause, after which rates equalize), Black African ancestry (which confers both higher prevalence and earlier onset), obesity, physical inactivity, high sodium intake, excessive alcohol consumption, and chronic stress are all independent risk factors.
Secondary Hypertension
The remaining 5 to 10 percent of hypertension is secondary to an identifiable underlying condition. The most common causes are chronic kidney disease, renal artery stenosis, primary aldosteronism (a hormonal condition causing excess aldosterone production), obstructive sleep apnea, and thyroid disorders. Secondary hypertension should be considered when blood pressure is difficult to control despite multiple medications, when it begins before age 30 without other risk factors, or when it worsens suddenly after previously being stable.
Medications can also raise blood pressure significantly. Non-steroidal anti-inflammatory drugs (NSAIDs like ibuprofen and naproxen), oral contraceptives, decongestants, certain antidepressants, stimulants, and high-dose steroids are among the most common pharmaceutical contributors. If you have hypertension and take any of these regularly, this is worth discussing with your physician.
Measuring Blood Pressure Correctly
Blood pressure is highly variable. It changes with activity, stress, anxiety, caffeine, full bladder, posture, and simply being in a medical environment. White coat hypertension, where blood pressure is elevated in a clinical setting but normal at home, affects 15 to 30 percent of people who have elevated readings in a doctor's office. This matters because white coat hypertension does not confer the same cardiovascular risk as sustained hypertension and may not require medication.
For an accurate reading: sit quietly for five minutes before measuring, feet flat on the floor, back supported, arm at heart level, no talking during the measurement. Take two readings two minutes apart and average them. Home blood pressure monitoring using a validated upper arm cuff provides far more useful data than occasional clinic readings. I routinely ask patients to take and record readings morning and evening for two weeks before making treatment decisions.
Consequences of Uncontrolled Hypertension
Heart Disease
Hypertension is the leading modifiable risk factor for coronary artery disease and heart failure. Sustained elevated pressure accelerates atherosclerosis, the buildup of plaque in arterial walls. Left ventricular hypertrophy increases the risk of dangerous arrhythmias including atrial fibrillation. Heart failure with preserved ejection fraction, a type of heart failure in which the heart muscle becomes stiff rather than weak, is heavily driven by longstanding hypertension.
Stroke
Hypertension is the single most important modifiable risk factor for stroke, responsible for approximately half of all strokes globally. Both ischemic stroke (caused by clot) and hemorrhagic stroke (caused by bleeding) are significantly more common with uncontrolled blood pressure. The risk of stroke rises proportionally with increasing blood pressure, and lowering blood pressure is the intervention with the strongest evidence for stroke prevention.
Kidney Disease
Hypertension damages the small blood vessels in the kidneys, impairing filtration. Over time, this leads to chronic kidney disease, which in turn worsens blood pressure control, creating a damaging cycle. Hypertensive nephropathy is one of the leading causes of end-stage kidney disease requiring dialysis. Blood pressure control is one of the most important interventions for slowing the progression of chronic kidney disease regardless of its initial cause.
Vision Loss
Hypertensive retinopathy, damage to the blood vessels of the retina caused by sustained elevated pressure, can impair vision and in severe cases lead to significant vision loss. Changes visible on fundoscopic examination also provide a window into the state of blood vessels throughout the body.
Treatment: Lifestyle First
For Stage 1 hypertension without high cardiovascular risk, lifestyle modification is the initial recommended approach. The evidence on lifestyle interventions is strong. Weight loss produces approximately 1 mmHg of systolic reduction per kilogram lost. The DASH diet (Dietary Approaches to Stop Hypertension), which emphasizes fruits, vegetables, whole grains, and low-fat dairy while limiting sodium and saturated fat, reduces systolic blood pressure by 8 to 14 mmHg. Sodium restriction to under 2,300 mg per day reduces systolic pressure by 5 to 6 mmHg. Regular aerobic exercise of 150 minutes per week reduces systolic pressure by 4 to 9 mmHg. Limiting alcohol to no more than one drink per day for women and two for men produces a further reduction.
These are not trivial effects. For a patient with Stage 1 hypertension, comprehensive lifestyle modification can produce reductions equivalent to a single blood pressure medication. The challenge is adherence. These changes require sustained commitment, and medication remains necessary for most patients with hypertension over time.
Blood Pressure Medications
The four main classes used as first-line therapy are thiazide diuretics, ACE inhibitors (or ARBs), calcium channel blockers, and beta-blockers. Selection depends on age, ethnicity, presence of other conditions, and medication tolerability. Many patients require two or more agents to reach target blood pressure, which should not be seen as a failure. The cardiovascular system is complex and resistant blood pressure often reflects multiple contributing mechanisms requiring multiple targets.
When to See a Doctor
If you do not know your blood pressure, finding out is the first step. If it is elevated on two separate occasions, evaluation and a management plan are appropriate. If your blood pressure has been difficult to control despite medication, evaluation for secondary causes may be warranted. JourneyDoctors cardiologists and internists can review your readings, assess your cardiovascular risk, and guide appropriate treatment. Consultations start at $19.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for diagnosis and treatment of any medical condition.
Get proper care
Ready to speak with a specialist?
If anything in this article sounds familiar, the right next step is a proper evaluation. JourneyDoctors connects you with a specialist in minutes. Consultations from $19.
See a specialist nowFrequently Asked Questions
Can high blood pressure go away on its own?
Primary hypertension is a chronic condition that does not resolve without intervention. However, meaningful lifestyle changes can lower blood pressure significantly, and in cases of Stage 1 hypertension, may normalize it without medication. Secondary hypertension can resolve if the underlying cause is treated, such as sleep apnea treatment or removal of an adrenal tumor. Blood pressure typically rises with age without ongoing intervention.
Is it safe to stop blood pressure medication if my readings normalize?
Not without physician guidance. Blood pressure often normalizes on medication because the medication is working. Stopping it typically causes readings to return to the pre-treatment level. In some patients who have made substantial lifestyle changes, a carefully supervised medication reduction may be appropriate. This should always be done with monitoring, not unilaterally.
What is a hypertensive crisis and what should I do?
A reading above 180/120 mmHg is a hypertensive crisis. If you have symptoms alongside this reading, such as chest pain, shortness of breath, severe headache, visual changes, or neurological symptoms, go to an emergency room immediately. If the reading is very high but you have no symptoms, sit quietly, recheck in 15 minutes, and contact your physician or seek urgent care.
Does stress cause high blood pressure?
Acute stress raises blood pressure temporarily through the sympathetic nervous system. Chronic psychological stress contributes to sustained hypertension through multiple mechanisms, including cortisol effects, unhealthy coping behaviors, and poor sleep. Managing chronic stress is a legitimate component of hypertension management, though it rarely normalizes blood pressure on its own in established hypertension.
How often should blood pressure be checked?
Adults with normal blood pressure should have it checked at every routine clinical visit, at minimum every two years. Adults with elevated readings or Stage 1 hypertension should be checked more frequently during the assessment period and monitored ongoing. Home monitoring with a validated cuff provides the most useful data for management decisions.
Written by
Dr. Adaeze Nwosu
Cardiology